
When people think about breast cancer treatment, they usually picture chemotherapy, radiation, and surgery. But for many of us, treatment doesn’t actually end there.
If you’ve been diagnosed with hormone receptor–positive breast cancer, chances are your doctor prescribed hormone blocking medication also called endocrine therapy or ovarian suppression medication. These medications can be life-saving because they help reduce the risk of cancer returning (sometimes by drastic percentages). But they also come with something many women aren’t fully prepared for – medical menopause and a host of horrible side effects.
For some women, it’s mild. For others, it can feel like their body changed overnight.
If you’re navigating this stage of treatment, here’s what you should know about hormone therapy, medical menopause, and what your oncologist may not have prepared you for. This is the reality many breast cancer survivors experience and I want you to have the tools needed to cope!
What Is Hormone Blocking Therapy?
Many breast cancers grow in response to hormones like estrogen and progesterone. When cancer cells have receptors for these hormones, they can use them as fuel to grow.
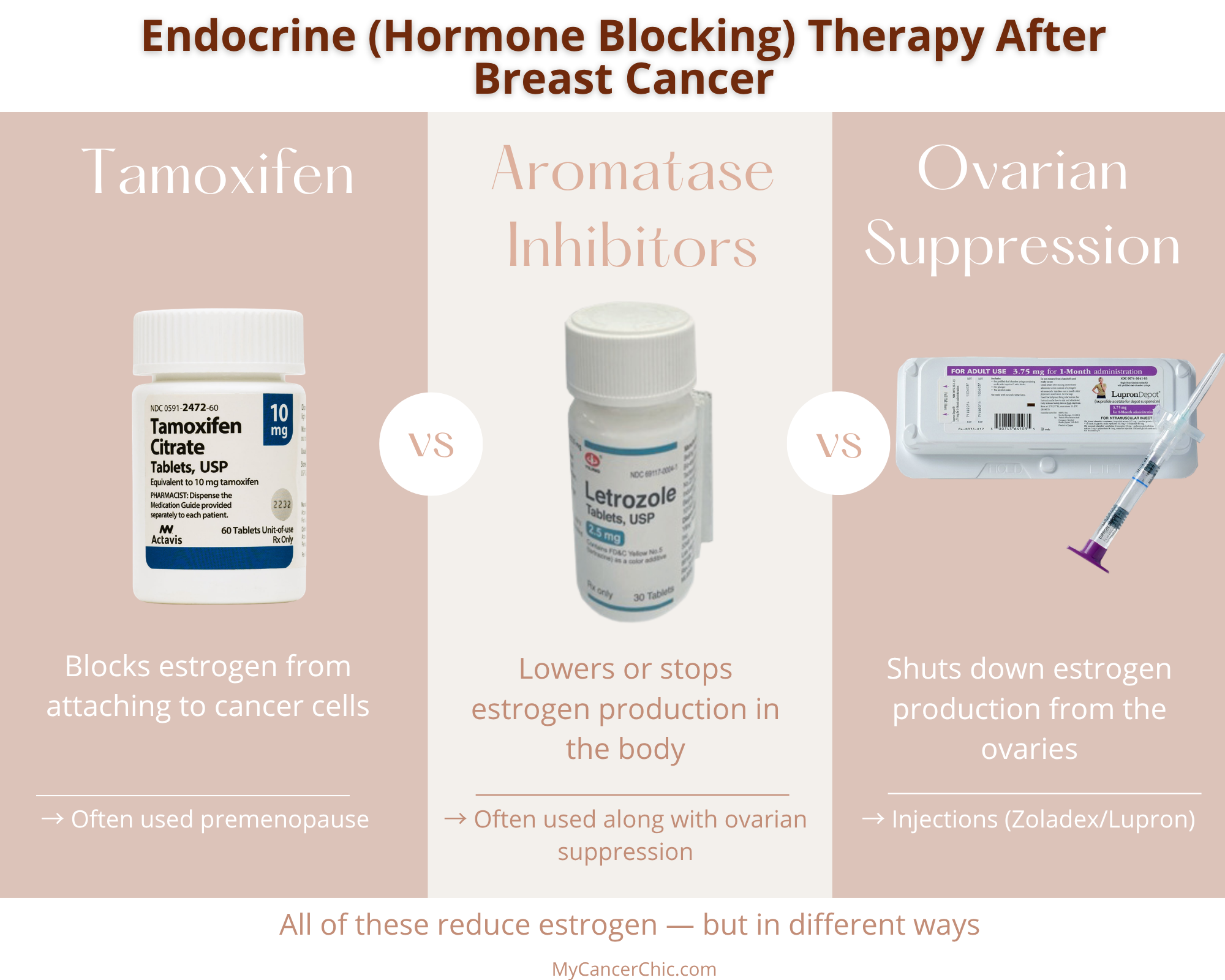
Hormone blocking therapy (also called endocrine therapy) works in a few different ways:
- Blocking estrogen from attaching to cancer cells (like Tamoxifen)
- Lowering the amount of estrogen the body produces (like aromatase inhibitors)
For premenopausal women, treatment may include ovarian suppression, which temporarily shuts down ovarian function so the body produces significantly less estrogen.
This can be done through:
- Monthly or quarterly injections (like Zoladex or Lupron)
- Surgery to remove the ovaries (in some cases)
Ovarian suppression is often combined with other hormone therapies — like Tamoxifen or aromatase inhibitors — to further reduce the risk of recurrence. The goal of all of these approaches is the same: to reduce the amount of estrogen available to fuel cancer growth.
For many breast cancer survivors, hormone therapy becomes part of long-term survivorship and is often prescribed for five to ten years after initial treatment. But when estrogen levels drop this quickly — especially with ovarian suppression — it can push the body into medical menopause, which is why many women experience symptoms like hot flashes, joint pain, sleep disruption, and mood changes.
For many of us, this is where treatment shifts from something temporary to something that becomes part of daily life for years. I literally went from a normal 27 year old to what felt like an 80 year old woman in 30 days!
The Most Common Hormone Blocking Medications
There are a few different types of hormone therapies used in breast cancer treatment, and which one you’re prescribed often depends on whether you are premenopausal or postmenopausal — or if your treatment includes ovarian suppression.
Aromatase Inhibitors (Often Used with Ovarian Suppression)
Aromatase inhibitors (AIs) work by blocking the aromatase enzyme, which the body uses to produce estrogen. This lowers overall estrogen levels in the body.
Some common ones include:
- Anastrozole
- Letrozole (I was on this for 5+ years along with Lupron for ovarian suppression)
- Exemestane
These medications are typically used for women who are already postmenopausal, when the body’s main source of estrogen comes from this enzyme process rather than the ovaries.
For premenopausal women, AIs are often prescribed in combination with ovarian suppression, which shuts down estrogen production from the ovaries.
This combination — an aromatase inhibitor plus ovarian suppression — has been shown in large clinical trials (like SOFT and TEXT) to further reduce the risk of recurrence in certain higher-risk patients compared to other hormone therapy options.
Tamoxifen (With or Without Ovarian Suppression)
Tamoxifen works differently. Instead of lowering estrogen levels, it binds to estrogen receptors on breast cancer cells and blocks estrogen from attaching.
It’s commonly prescribed for premenopausal women and can also be used after menopause.
In some cases, Tamoxifen is used on its own. In others, it may be combined with ovarian suppression to further reduce estrogen’s impact on the body.
What Is Medical Menopause?
Medical menopause happens when treatments force the body into menopause earlier than it would naturally occur. Unlike natural menopause, which usually happens gradually over time, medical menopause can happen almost overnight. This is especially common for younger women who are suddenly thrown into menopause because of cancer treatment.
Estrogen affects many systems throughout the body, including temperature regulation, bone health, mood, sleep, and sexual health. When those levels drop quickly, the body reacts with many of the same symptoms seen in natural menopause. Sometimes those symptoms are even more intense.
Common Symptoms of Medical Menopause
Every woman’s experience with hormone therapy is different, but there are some common symptoms many survivors report. For many breast cancer survivors, these symptoms can be frustrating because they affect daily life — work, relationships, sleep, and overall quality of life. And sometimes people around us don’t realize we’re still dealing with treatment side effects long after chemo or radiation has ended.
- Hot flashes / Night sweats
- Fatigue
- Joint pain or stiffness
- Vaginal dryness & pain during intercourse
- Mood changes
- Brain fog
- Sleep disruptions
- Loss of libido
Some women also notice changes in their skin, hair, or weight. Tamoxifen in particular is known to cause weight gain

What This Actually Feels Like (From My Community)
One thing I’ve learned in survivorship is that sometimes the most helpful insights don’t come from a pamphlet — they come from other women living it in real time. My friend Kim actually wrote one of the first guest posts on the topic of hormone blocking therapy many years ago for My Cancer Chic, and she captured the day-to-day reality of hormone therapy and medical menopause so honestly. While Kim is no longer with us here on earth I know she would LOVE to have her words to live on when it comes to this tough topic and helping others navigate!
I hope her words of insight help you feel less alone as you navigate the symptoms of hormone blocking therapy.
What to Expect with Ovarian Suppression Injections (Zoladex or Lupron)
Kim shares:
“The Zoladex injection is administered every 28 days and comes as a preloaded syringe with a slow-release tablet. My oncologist uses a numbing spray, but since it only affects the top layer of skin, you still feel the needle — and at 16 gauge, it’s no joke. Thankfully, my doctor is quick, and it’s over before I can really think about it. I’ve also heard good things about Emla cream as another option to help numb the area.”
Did you know you can get approval to do your injections from home?! I was on Lupron for over five years, and eventually the logistics became just as exhausting as the treatment itself. After a few years of going into the office every month, I worked with my care team to get approved for at-home injections, and my husband was trained to administer them. This is becoming more common now, but it can take some insurance coordination — definitely something worth asking about if you’re on long-term ovarian suppression.
Hot Flashes
Hot flashes are one of the most common hormone therapy side effects, especially when estrogen levels drop quickly during medical menopause.
Kim shares:
“I used to always be cold, wrapped in a blanket. Now, hot flashes hit and it feels like my body goes from 0 to 100 in seconds. I get red-faced, uncomfortable, and it can be really agitating. I’ve learned to layer clothes and keep a fan nearby — especially at night.”
Anxiety and Panic Attacks
Hormonal changes don’t just affect the body — they can also have a significant impact on mental health, including increased anxiety and panic symptoms.
Kim shares:
“I never experienced anxiety like this before. It can show up out of nowhere — driving, at dinner, or lying in bed. It feels like agitation in my body, shortness of breath, and racing thoughts I can’t quiet. I’m working on managing it with yoga and breathing exercises, but it’s still a work in progress.”
Even now, years later, I still experience anxiety and panic attacks at times. The difference now, is I’ve built tools to manage them — including consistent medication, therapy and coping strategies I consistently come back to. It doesn’t disappear overnight, but it does become more manageable.
Brain Fog and Difficulty Concentrating
Cognitive changes, often referred to as “brain fog,” are another common side effect of hormone therapy and medical menopause.
Kim shares:
“Even trying to find the right words can feel hard. My brain feels foggy, and I get frustrated repeating myself or forgetting things. It’s not that I’m not listening — I just can’t retain information the way I used to.”
Insomnia
Sleep disruption is incredibly common during hormone therapy, especially with night sweats and hormonal fluctuations affecting your sleep cycle.
Kim shares:
“Sleep has been one of the hardest parts. I’ve stayed up until sunrise more times than I can count. I’ve tried everything — melatonin, magnesium, meditation — and sometimes the only option is medication, even though I wish I didn’t need it.”
Joint Pain and Body Aches
“At night, I feel a deep ache in my legs, and in the morning my hands feel stiff and need to be stretched carefully. Sometimes I joke that I feel like I need WD-40 for my joints.
What helps: Epsom salt baths, walking, and yoga to keep things moving.” – Kim
Bone Health and Long-Term Side Effects
Long-term hormone therapy — especially aromatase inhibitors — can impact bone density and increase the risk of osteoporosis and fractures.
Tamoxifen is a little more nuanced. In premenopausal women, it can contribute to bone loss, while in postmenopausal women it can actually help preserve bone density.
Kim shares:
“Before starting treatment, I had a bone density scan to check for osteoporosis risk. Aromatase inhibitors can increase bone loss, and a few months in, I developed arthritis in my thumb. I’m now taking calcium and vitamin D, and my doctor has recommended additional medications to protect my bones — but like everything, it’s another decision with trade-offs.”
Bone health is an important topic for young cancer patients and your doctor should do a baseline scan before hormone blocking therapy begins. Many doctors will monitor bone loss from endocrine therapy through annual bone density scans and comparison over time.
Weight-bearing movement — like walking, strength training, or even light resistance work — can help support bone health and is often encouraged during treatment. For some women, especially those at higher risk for bone loss, doctors may also recommend medications or injections (like bisphosphonates or similar therapies) to help protect bone density.
Vaginal Dryness, Libido, and Intimacy Changes
Hormone therapy can also affect sexual health in ways that aren’t talked about nearly enough. Lower estrogen levels can lead to vaginal dryness, discomfort, and changes in libido — all of which can impact both physical intimacy and emotional connection.
This is something so many survivors experience but don’t always feel comfortable talking about.
I go much deeper into this in my post on sex and intimacy after cancer, including what’s helped me and what to expect.
Why Hormone Therapy Is Still Important
Even though hormone therapy can be challenging, it plays a very important role in breast cancer treatment and long term survival rates. Studies show that hormone blocking medications significantly reduce the risk of hormone-positive breast cancer returning. That’s why oncologists often recommend staying on these medications for 5-10 years after active treatment.
How I Made Decisions About Hormone Therapy
One of the hardest parts of starting hormone therapy wasn’t just the side effects — it was figuring out what the right treatment plan was for me and the timing for when to take a break to start a family. I go into that more deeply into my fertility journey in this podast episode with Dr. Teplinsky.
There isn’t a one-size-fits-all approach, especially for younger, premenopausal women. Kim’s doctor encouraged her to look into the SOFT and TEXT trials to better understand the options and feel more confident in her decision.
These studies looked at different types of hormone therapy for premenopausal women and found that:
- Taking an aromatase inhibitor (AI) + ovarian suppression showed greater benefits for higher-risk patients
- Compared to Tamoxifen + ovarian suppression
That doesn’t mean one option is “right” for everyone — but it can help you understand why certain combinations are recommended based on risk level. For many people, having that context made a really overwhelming decision feel a little more grounded.
What Is the Breast Cancer Index (BCI) Test?
Another tool that can sometimes be part of this decision-making process is the Breast Cancer Index (BCI) test. The BCI Test is the only genomic test recognized by leading oncology guidelines to predict which patients are likely to benefit from continuing anti-estrogen therapy after the first five years of treatment.
The BCI test provides two results to help you make a personalized decision about the length of your anti-estrogen therapy:
- A clear ‘yes’ or ‘no’ answer to whether an additional five years of anti-estrogen therapy is likely to reduce your risk of recurrence.
- Your individual percent risk of metastatic recurrence after the five year mark, if you take five years of anti-estrogen therapy versus ten.
For many women, especially those nearing the end of their initial hormone therapy plan, this test can help guide the decision of whether to continue treatment longer. The hope is that it will soon be available to inform decision making sooner as well. It’s worth asking your doctor about — especially if you’re trying to weigh the long-term benefits of starting or staying on hormone therapy.
In my case the test confirmed another 5 years on endocrine therapy would be beneficial and that data led to the decision for us to have another child before I extended my treatment. At the end of the day, hormone therapy decisions are deeply personal — and often come down to balancing risk reduction with quality of life.
Having access to research, testing, and open conversations with your care team can make a big difference in feeling confident in your plan.
The Emotional Side of Medical Menopause
Something that doesn’t get talked about enough is the emotional side of medical menopause. When perimenopause or menopause happens naturally later in life, it’s generally expected. It doesn’t mean it’s easy but it usually happens gradually with some warning signs.
But when it’s caused by cancer treatment — sometimes in your 20s or 30s — it can feel like your body has been taken over suddently.
Many women experience emotional and psychological feelings of:
- loss of control
- grief over fertility changes
- frustration with physical symptoms
- identity shifts around aging or sexuality
These feelings are completely valid and I know I went through an entire rollercoaster or emotions processing my side effects and symptoms at many times throughout the last 10 years of treatment. It’s OK to be angry and frustrated this is the experience we are going through while also recognizing the long-term benefit of the treatment.

Managing Symptoms of Medical Menopause
While hormone therapy symptoms can be difficult, there are many interventions to support and in recent years as menopause in general gets more attention there are even new drugs on the market to address some of the side effects such as hot flashes and night sweats.
Non-Hormonal Option for Hot Flashes
The non-hormonal medication Veozah was FDA-approved to treat moderate to severe hot flashes. Unlike traditional hormone replacement therapy, this medication works by targeting the brain’s temperature regulation and does not contain estrogen — which makes it an important option for some breast cancer survivors.
That said, it’s not right for everyone, and it’s important to talk with your oncology team about whether it’s a safe and appropriate option for you.
Many doctors also recommend managing symptoms with lifestyle strategies such as:
- regular movement and exercise
- sleep aids & sleep hygiene
- stress management, mediation and therapy
- balanced nutrition + GLP1s
- bone health support through calcium and vitamin D and load bearing activity
- vaginal estrogen and other interventions for sexual health and intimacy concerns
The most important thing is to talk openly with your care team about what you’re experiencing. There may be options that can help.
One of the hardest parts of breast cancer survivorship — especially when you’re on long-term hormone therapy — is that the outside world often thinks treatment is “over.”
But many of us know that’s not the reality. We’re still navigating medications, side effects, and emotional healing long after active treatment ends. If you’re experiencing medical menopause, or feeling the impact of endocrine therapy or ovarian suppression, please know you’re not alone in this.
So many women are walking this same path — adjusting, learning, and redefining what life after cancer looks like. I hope this guide brought you insight, resources, and a sense of comfort in the process.
